Estimated readtime: 6 min
This blog is also available in Portuguese, Spanish, and Russian.
Authors: Dhanusha Nirmani, Alex Regan, Annette Ozaltin, Ravi P. Rannan-Eliya
The Linked Immunisation Action Network (Linked) brought together nearly 60 immunisation and primary health care practitioners from 10 middle-income countries (MICs) – Armenia, Azerbaijan, Bhutan, Georgia, Indonesia, Kiribati, Sri Lanka, Timor-Leste, Uzbekistan, and Vietnam – for a virtual learning exchange in July on “Benefits and Implementation Considerations for Electronic Immunisation Registries”. Hosted by the Institute for Health Policy (IHP), the learning exchange responded to critical challenges reported by MICs in the tracking of routine immunisation and in the roll out of COVID-19 vaccines, and recent experience of several countries in leveraging electronic immunisation registers (EIRs) to support expansion of vaccination coverage.
EIRs are a transformational step-up from existing digital vaccine information systems, such as the DGHIS2, that help healthcare managers track vaccine delivery. They differ by tracking vaccinations not at the provider or program level, but at the level of individuals, and throughout the life course from birth to death. By being oriented towards individuals, they can integrate the tracking of coverage across different providers or even public and private sectors, and be more responsive to citizen’s needs, such as providing vaccine certificates on request.
When put in place, they help enhance the performance of immunisation programmes and can complement other immunisation systems, such as those for supply chain, surveillance, and monitoring of Adverse Events Following Immunisation (AEFI). They can also provide real time monitoring of vaccination coverage gaps, which traditional systems often require surveys for. Before the COVID-19 pandemic, only a few countries had adopted or taken initial steps to establish EIRs to track their routine immunisation activities, such as Australia, Canada, Italy, several Latin American countries, the Nordic countries, Tanzania, and Vietnam. During the pandemic, many countries had to create new systems to track COVID-19 vaccinations to support issue of travel certificates or vaccine passports, but countries, which had EIRs, such as Australia and Vietnam, were able to leverage their existing systems to take on this new challenge, integrating the tracking of COVID-19 vaccines into a single system for all vaccines.
The Linked learning exchange highlighted the potential benefits and lessons learned from using EIRs, showcased the experience of one country with a long- established EIR and two countries with less mature systems, focused on the implementation challenges in adoption and evolution of EIRs, and provided tips on how to facilitate a smooth transition from an existing paper-based system to an EIR.
A presentation by Dr. Meru Sheel, Associate Professor at the Sydney School of Public Health at the University of Sydney, introduced the concept of EIRs and gave a detailed overview of the Australian Immunisation Register (AIR). Established in 1996 and maintained by Services Australia on behalf of the Australian Government Department of Health, the AIR has evolved over time, first capturing essential data at the individual level for childhood vaccines <7 years, then expanding 20 years later to include all ages, with HPV register data finally incorporated a couple years after that, and now tracking COVID-19 vaccinations. Dr. Sheel described the benefits of EIRs:
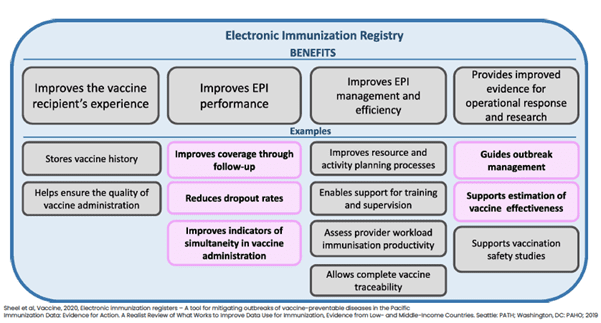
She also specified that EIRs allow for both individual level follow-up and program evaluation for population impact—improving coverage estimates, targeting to reach zero-dose children and other hard-to-reach populations, permitting effectiveness and cost-effectiveness analysis, and monitoring of AEFI. Dr. Sheel argued that EIRs can improve vaccine coverage and strengthen immunisation programmes, but they often take a long time to mature. To make the most out of new EIRs, she provided a number of recommendations, including the use of a unique identifier, institution of data quality control processes, and alignment with other components of immunisation information systems. For countries that established COVID-19 registries, she urged them not to “waste a crisis” and to use program and process evaluation to help develop these further to build integrated systems to cover routine child immunisation.
The learning exchange also featured presentations on Vietnam’s EIR established over a decade ago, and Bhutan’s COVID-19 registry established during the pandemic. Mr. Sang Dao Dinh, IDEAL-Vietnam Team Lead representing PATH Vietnam, shared Vietnam’s experience of using EIRs for both routine and COVID-19 vaccinations. After a pilot phase beginning in 2012, Vietnam’s Immunisation Registry Module, called the National Immunisation Information System (NIIS), was launched nationwide in 2017 by the Ministry of Health. This system features an immunisation tracker that relies on barcode scanning, SMS reminders, and e-immunisation cards. The system has helped increase on-time vaccination and reduce dropout rates. As the system has evolved over time, the latest focus has been to increase uptake among providers, improve data quality and data use, and transition to paperless immunisation records. Hardware limitations prevented the system from taking on COVID-19 vaccination, but the core system was cloned on to a larger infrastructure for COVID-19 vaccination. Key facilitators for establishment of an EIR included commitment, prioritization and support from both the government and other partners, training and technical support from organizations like PATH, and small pilots informing nationwide scale-up. Key challenges included lack of resources, supervision, poor infrastructure, and inconsistent data quality.
Mr. Garab Dorji, Chief ICT Officer from the ICT Division of the Ministry of Health Bhutan, shared Bhutan’s experience using a COVID-19 registry. Previously, Bhutan had used a paper-based system and other digital platforms to track vaccinations. The new Bhutan Vaccine System utilizes an open-source digital platform to track vaccine doses at the individual level and generate vaccination certificates. Residents are either enrolled automatically, through a link to the civil database and the immigration database, through their providers, or through an online portal. Different modules allow provider recording of vaccine doses, and provider/self-reporting of AEFIs, while a mobile app gives individuals access to their vaccination history. Key facilitators of the establishment of a COVID-19 registry in Bhutan included the opportunity to leverage COVID-19 resources, national prioritization, stakeholder collaboration, and a favorable IT environment through a national eGov policy and eHealth strategy. Key challenges included poor connectivity, an unstable system, inconsistent data and inventory, inadequate training, and user acceptance of new technology. Going forward, Bhutan plans to incorporate routine vaccines into the system and integrate the registry with other global VC, DHIS2, epi GPS tracker, HIS, and others.
Participants and presenters acknowledged that the virtual exchange just scratched the surface on the topic of EIRs, and they requested more in-depth learning on the introduction and implementation of EIRs. The questions and discussion centered around practical implementation considerations, such as governance roles and responsibilities for EIRs, the cost and time to establish EIRs, at which levels to implement EIRs and for which provider types, how to integrate EIRs with other digital information platforms, and how to ensure data quality and address denominator challenges. The Linked network will aim to reconvene practitioners on this topic as a means to strengthen the capacity of immunisation programmes to collect, analyze, interpret, and act on their data. Indeed, updated, reliable, and comprehensive information on immunisation coverage is critical for restoring routine immunisation services, identifying and targeting zero-dose children and missed communities, and organizing effective catch-up campaigns.
The presentations and video recording of the learning exchange can be found here on our website. Additional resources for further reading on EIRs are shared below. Make sure you stay updated on the latest network offerings and learnings by signing up for our email list!
Additional Related Resources:
Danovaro-Holliday, M. C., Ortiz, C., Cochi, S., & Ruiz-Matus, C. (2014). Electronic immunisation registries in Latin America: progress and lessons learned. Rev Panam Salud Publica, 35(5-6), 453-457.
Pan American Health Organization. (2017). Electronic Immunisation Registry: Practical Considerations for Planning, Development, Implementation and Evaluation. Washington, D.C.: PAHO.
Pebody, R. (2012). Vaccine registers – experiences from Europe and elsewhere. Eurosurveillance, 17(17). doi:http://www.eurosurveillance.org/
Rannan-Eliya, R. P. (2021). National Immunisation Registers – Recent Experiences in Supporting COVID-19 Vaccination and Integrating Adult and Child Vaccination Delivery. Retrieved from https://www.linkedimmunisation.org/blog/national-immunisation-registers-recent-experiences-in-supporting-covid-19-vaccination-and-integrating-adult-and-child-vaccination-delivery/
Secor, A. M., Mtenga, H., Richard, J., Bulula, N., Ferriss, E., Rathod, M., . . . Carnahan, E. (2022). Added Value of Electronic Immunisation Registries in Low- and Middle-Income Countries: Observational Case Study in Tanzania. JMIR Public Health Surveill, 8(1), e32455. doi:10.2196/32455
Sullivan, E., Masood, T., Javed, W., Bagshaw, K., Ollis, S., Regmi, P., & Gardezi, S. M. A. (2020). Electronic immunisation information systems: a case report of lessons learned from implementation in Pakistan. mHealth, 6, 31-31. doi:10.21037/mhealth.2020.01.07